
May 28, 2026
Bone and Cartilage Injury Rehabilitation: Why Biology Determines Your Timeline — Not Your Clinic’s Protocol Sheet
“My fracture healed on the X-ray three months ago. So why does my joint still feel wrong?” — The most important answer to this question is one most clinics never give. This is ours.
The problem with standard bone and cartilage recovery advice
Most patients recovering from bone and cartilage injuries are given one of two instructions: rest until it heals, or follow a fixed-week protocol. Both approaches share the same fundamental flaw — they treat tissue healing as a calendar event rather than a biological process.
Bone and cartilage are structurally and biologically different tissues. They heal through different mechanisms, respond to load in different ways, and fail in different ways when rehabilitation is poorly timed. Treating them with the same generic protocol — or no protocol at all — is one of the primary reasons patients reach the six-month mark still not functioning the way they expected to.
At Movementology, rehabilitation after bone and cartilage injury is delivered through the Arthrorehab programme — a structured clinical methodology built around tissue biology, criteria-based progression, and precise load management. You advance through recovery when your tissue demonstrates readiness. Not when the date says so.
Why bone and cartilage heal so differently — and why it matters for your rehabilitation
🦴 Bone
Well-vascularised tissue with a robust four-stage healing process. Responds predictably to load — in fact, requires mechanical stimulation to mineralise properly. Can heal completely with the right rehabilitation sequencing.
🔵 Articular cartilage
Avascular — no direct blood supply. Receives nutrients entirely through synovial fluid exchange driven by joint movement and cyclic loading. Has very limited capacity for self-repair. Deteriorates silently if rehabilitation is delayed, unstructured, or poorly loaded.
This difference is clinically critical. Bone heals through biology — cartilage heals through movement. If your joint is immobilised for too long, cartilage matrix integrity degrades. If it is loaded too aggressively too early, both tissues are at risk. The window of optimal loading is specific, and it requires a clinician who understands tissue biology — not just symptom management.
MOVEMENTOLOGY CLINICAL PRINCIPLE
Radiological healing and functional healing are two entirely different milestones. An X-ray showing callus formation tells you the bone has bridged. It tells you nothing about proprioceptive recovery, muscular symmetry, joint load tolerance, or cartilage integrity. At Movementology, we assess all four — not just the image.
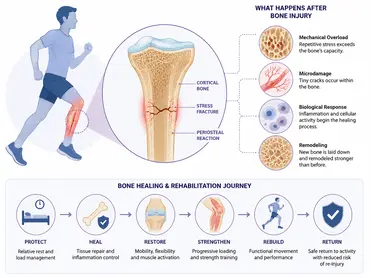
The four stages of bone healing — and what rehabilitation must do at each one
The bone injury healing process follows four biologically distinct stages. Each one has a different tissue profile, different load tolerance, and different rehabilitation requirement. Rushing any stage increases re-injury risk. Immobilising too long at any stage accelerates muscle atrophy, joint stiffness, and proprioceptive loss.
| HEALING STAGE | TIMEFRAME | EXIT CRITERIA — WHAT MUST BE DEMONSTRATED |
| Inflammatory | Days 1–7 | Swelling controlled, neurovascular status confirmed, pain manageable without complete immobilisation, soft tissue circulation maintained |
| Soft callus | Weeks 1–3 | Gentle range of motion initiated, neuromuscular activation restored in surrounding musculature, no pathological loading at fracture site |
| Hard callus | Weeks 3–8 | Progressive axial loading tolerated without pain, joint range of motion benchmarks met, muscle activation symmetry measurable |
| Bone remodelling | Weeks 8–16+ | Full functional range of motion restored, progressive resistance loading tolerated, limb symmetry index tracked and improving |
| Return to activity | Week 16+ | Single-leg loading symmetry ≥85%, functional movement screening passed, sport/occupation-specific load tolerance confirmed, no joint effusion under load |
CRITERIA-BASED PROGRESSION — THE ARTHROREHAB STANDARD
At Movementology, no patient advances to the next phase of rehabilitation because a week has passed. They advance because their tissue has demonstrated, through objective clinical assessment, that it is ready for the next level of demand. This single principle is what separates structured tertiary rehabilitation from standard physiotherapy — and it is what makes the difference between full recovery and managed decline.
Cartilage injury rehabilitation — the most mismanaged tissue in orthopaedic recovery
Articular cartilage is the tissue most commonly undertreated in standard rehabilitation. Because it has no blood supply and no nerve endings in its deeper layers, cartilage damage is often painless in its early stages — and by the time symptoms appear, significant matrix degradation has already occurred.
Cartilage wear and tear symptoms — joint stiffness, reduced range of motion, crepitus, intermittent swelling — are not the beginning of the problem. They are evidence that the problem has been developing, undetected and unmanaged, for some time.
What cartilage actually needs to heal
Cartilage receives nutrition through cyclic compression and decompression — the mechanical pumping action of joint loading that drives synovial fluid exchange into the cartilage matrix. This means cartilage requires movement and controlled load to maintain integrity. Prolonged rest or immobilisation does not protect cartilage. It starves it.
- Controlled axial loading is the primary driver of cartilage nutrition — initiated carefully, progressed precisely
- Synovial inflammation management is a clinical prerequisite — untreated synovitis directly reduces cartilage nutrition and accelerates matrix loss
- Progressive mechanical stimulation — not aggressive, not passive. The load window for cartilage repair is narrow and requires specialist clinical judgment to manage
- Regenerative interventions — at Movementology, PRP and orthobiologic therapies are integrated into cartilage rehabilitation protocols where tissue biology supports their use, always paired with a structured loading programme
THE MOST COMMON CARTILAGE REHABILITATION MISTAKE
Treating cartilage injury with rest alone. Cartilage has no vascular supply — it cannot heal through biological repair pathways the way bone can. Without structured mechanical stimulation, cartilage matrix integrity continues to degrade even while the patient is “resting.” Early, structured, biology-driven rehabilitation is not optional for cartilage. It is the treatment.
Bone stress injuries — a category that standard rehabilitation consistently underestimates
Bone stress injuries — stress reactions and stress fractures — deserve specific attention because they are among the most mismanaged presentations in orthopaedic rehabilitation. They are almost exclusively caused by load that exceeds the bone’s current adaptive capacity: too much volume, too little recovery, or a sudden change in training surface or intensity.
The critical clinical insight is this: a stress fracture is not simply a fracture that happened to be caused by activity. It is evidence of a bone remodelling imbalance — where osteoclastic resorption is outpacing osteoblastic formation. That imbalance requires a rehabilitation programme that addresses the underlying cause, not just the fracture site.
Movementology bone stress injury assessment — what we evaluate beyond the fracture
- Training load history — volume, intensity, surface, footwear, and rate of progression
- Nutritional status — calcium, vitamin D, and overall energy availability (RED-S screening where indicated)
- Bone density considerations — particularly in female athletes and masters-level competitors
- Biomechanical load distribution — gait analysis, landing mechanics, foot posture
- Return-to-load criteria — graded programme with objective milestones, not time-based clearance
At Movementology, bone stress injury rehabilitation is not managed with rest and a follow-up appointment. It is managed with a full clinical assessment of why the injury occurred — and a structured programme that addresses every contributing factor before return to full load is sanctioned.
What immobilisation destroys — and how we restore it
Immobilisation is sometimes clinically necessary. But it produces predictable, measurable consequences that structured rehabilitation must address systematically. At Movementology, we assess and treat each of these as distinct clinical deficits — not as a single “recovery” process.
- Muscle atrophy: Type II muscle fibre loss begins within 72 hours of immobilisation. Strength deficits of 20–30% can accumulate within weeks. Progressive resistance rehabilitation rebuilds cross-sectional area and tendon stiffness — but only when loading is precisely calibrated to the tissue’s current tolerance
- Proprioceptive deficit: The mechanoreceptors embedded in joint capsule, ligaments, and periarticular tissue are disrupted by immobilisation — not just by injury. Neuromuscular re-education is a distinct, non-negotiable component of the Arthrorehab protocol
- Joint stiffness: Connective tissue contracture and synovial fluid changes during immobilisation produce stiffness that will not resolve through passive stretching alone. Mobility restoration requires progressive, load-appropriate joint movement — guided by range-of-motion exit criteria, not comfort
- Altered movement mechanics: The compensatory patterns established during immobilisation — offloading the injured limb, altered gait, trunk stabilisation changes — become habitual within weeks. These patterns must be assessed and corrected explicitly, or they persist long after tissue healing is complete
The technology Movementology uses — and the clinical reasoning behind each choice
Movementology is equipped with technology specifically selected for bone and cartilage rehabilitation at the tertiary level. Every technology is used within the Arthrorehab protocol — meaning its application is determined by clinical criteria, not by availability.
BTL Zero Gravity Treadmill
Allows full gait-cycle rehabilitation — heel strike through push-off — with up to 80% body weight offloaded. Critical for bone stress injury recovery and post-fracture rehabilitation where axial load must be controlled precisely. Preserves neuromuscular gait patterns and cardiovascular conditioning during restricted weight-bearing phases.
Storz Focused Shockwave (Storz Medical)
Delivers acoustic energy to stimulate cellular repair at the tissue level — promotes extracellular matrix regeneration in cartilage, accelerates callus remodelling in delayed bone healing, and addresses concurrent tendon pathology. Storz Medical sets the global standard for this technology.
Super Inductive System
Deep neuromuscular stimulation for muscle groups that cannot be effectively activated by surface approaches. Used specifically during the early rehabilitation phase when pain-inhibition limits voluntary quad and hip stabiliser activation — a common post-fracture clinical barrier.
Class IV Laser (Japanese unit)
Photobiomodulation to accelerate tissue repair, manage localised inflammation, and support cartilage matrix regeneration. Used during the inflammatory and early callus stages — timed precisely within the Arthrorehab protocol for each tissue type and healing stage.
The clinical principle behind every technology decision at Movementology is the same: the tool serves the protocol, not the other way around. Any clinic can acquire equipment. What cannot be acquired is the clinical judgment — built over 24 years of specialist practice — to know when to use it, at what dose, in what sequence, and when not to use it at all.
Return to activity — what clearance means at Movementology
Return to full activity after bone and cartilage injury is not a date on a timeline. It is a set of objective clinical criteria that must all be met before we sign off. For patients returning to sport, occupation, or high-load activity, the standard is uncompromising — because the consequence of premature return is re-injury and, in the case of cartilage, progressive joint deterioration that is difficult to reverse.
Movementology return-to-activity clearance criteria — bone and cartilage
- Limb symmetry index ≥85% on strength and functional testing (≥90% for high-load sport return)
- Full pain-free range of motion equal to the unaffected side
- Single-leg loading symmetry confirmed — no compensatory movement patterns under functional load
- No joint effusion at rest or with activity-level loading
- Functional movement screening passed — sport or occupation-specific where relevant
- Bone stress injury: graded return-to-load programme completed with no symptom recurrence
- Cartilage cases: absence of effusion and clinical stability under progressive load confirmed by lead clinician
Patients who do not meet these criteria receive a precise programme targeting the specific deficit — not a generic “keep going” instruction. That clinical honesty is what tertiary rehabilitation looks like in practice.
Whether you are recovering from a fracture, managing cartilage damage, or dealing with a bone stress injury that hasn’t responded to standard treatment — Movementology is built for cases the standard system finds difficult. Dr. Padmanaban and the Arthrorehab clinical team will give you a biology-driven assessment and a criteria-based recovery programme built around your specific injury, your tissue stage, and your functional goals.
Book your assessment at Movementology
Frequently asked questions
- My fracture healed on X-ray months ago — so why does my joint still feel wrong?
Because radiological healing and functional healing are two different milestones. An X-ray confirms osseous continuity — that the bone has bridged. It tells you nothing about the state of the surrounding cartilage, the proprioceptive deficit that accumulated during immobilisation, the muscle symmetry loss, or whether your movement patterns have been altered by the compensatory habits you developed during recovery. At Movementology, a full functional assessment examines all of these — not just the imaging. This is one of the most common presentations we see: patients whose bone healed on schedule but whose function never did. - Can cartilage damage be treated without surgery?
For many grades of cartilage damage, yes. Structured criteria-based rehabilitation, precision load management, regenerative interventions (PRP, orthobiologics where appropriate), and the technology available at Movementology can achieve significant cartilage recovery and functional restoration without surgical intervention. The key is early, structured clinical management — not rest and observation. The later cartilage damage is treated, the more limited the non-surgical options become. If you have been told cartilage damage is something to “manage and monitor,” a tertiary assessment at Movementology may give you a very different clinical picture. - What is a bone stress injury and how is it different from a regular fracture?
A bone stress injury — stress reaction or stress fracture — results from cumulative load that exceeds the bone’s adaptive capacity, rather than a single traumatic event. The critical difference for rehabilitation is that a stress fracture is evidence of a remodelling imbalance: bone is being broken down faster than it is being rebuilt. That imbalance has causes — training load, nutrition, biomechanics, bone density — and those causes must be addressed as part of rehabilitation, or the injury will recur. At Movementology, bone stress injury rehabilitation includes a full assessment of contributing factors, not just management of the fracture site. - Why does joint stiffness persist even after a bone injury heals?
Because joint stiffness after fracture healing is not a bone problem — it is a soft tissue problem. Connective tissue contracture, synovial fluid changes, muscle weakness, and altered neuromuscular patterns all develop during immobilisation and do not resolve spontaneously once the fracture heals. These are distinct clinical deficits that require structured mobility restoration therapy, progressive loading, and neuromuscular re-education. At Movementology, persistent post-fracture stiffness is assessed as a separate clinical problem with its own criteria-based resolution pathway. - I’ve had a bone or cartilage injury that hasn’t responded to standard physiotherapy. What can Movementology offer that’s different?
This is the patient Movementology was built for. Standard physiotherapy is excellent for straightforward presentations. Bone and cartilage injuries that haven’t responded — whether because of inadequate load management, missed contributing factors, incomplete immobilisation sequencing, or simply insufficient clinical depth — require tertiary-level assessment and a different approach entirely. The Arthrorehab programme, delivered by Dr. Padmanaban and the Movementology clinical team, combines 24 years of specialist clinical experience, criteria-based progression, and technology that most rehabilitation centres in Bengaluru simply do not have access to. If the standard system hasn’t resolved your problem, we would like to see you.
Dr. Padmanabam Sekaran P.T
Chief Physiotherapist, Lead Consultant – Advanced Orthopedic Rehabilitation